SOLVING NIGHTTIME URINATION
A Diet & Lifestyle Problem, Not a Bladder Problem

Solving Nighttime Urination
Every single night, 50 million Americans are jolted awake by the urgent need to use the bathroom, not just once but two, three, or even five times, disrupting their sleep and leaving them exhausted by morning. What doctors often fail to mention during appointments is that in 80% of these cases, the bladder itself is perfectly healthy and not the root cause of the problem, meaning the pills, supplements, and herbs targeted at the prostate or bladder are addressing the wrong organ entirely. This video from Dr. Waterling challenges the conventional narrative, emphasizing that the medical system profits from keeping patients sick rather than curing them, and promises revelations not shared in clinic waiting rooms. Imagine it’s 3:00 a.m., your home is silent, and you’ve finally drifted into deep, restorative sleep only for a faint signal to pull you back to consciousness; you try to ignore the building pressure, but eventually, you throw off the covers, stumble to the cold floor, and shuffle to the bathroom like a zombie, squinting in the harsh light. After relieving yourself, sleep evades you as your mind races with worries about work, finances, and family, and just as you nod off again, it happens once more, leaving you shattered and reliant on coffee to get through the day. The doctor sees this exhaustion in countless patients who resign themselves to it as an inevitable sign of aging, but this is a dangerous lie that must be debunked immediately.
Why Nocturia Is Not Normal and Its Serious Health Impacts
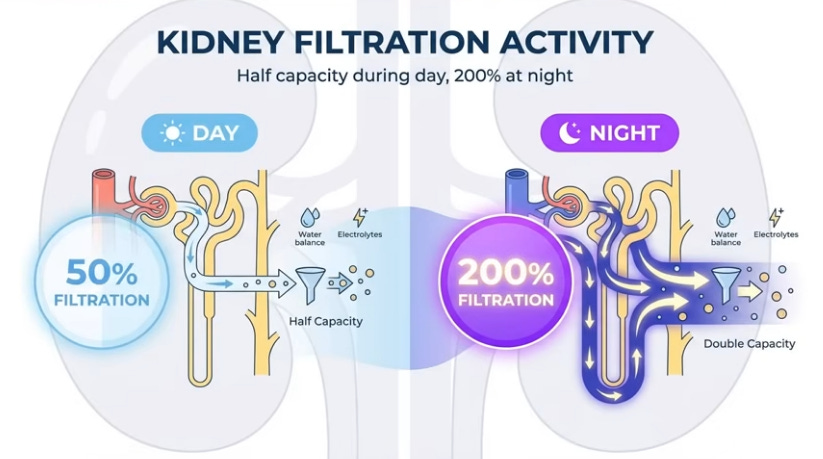
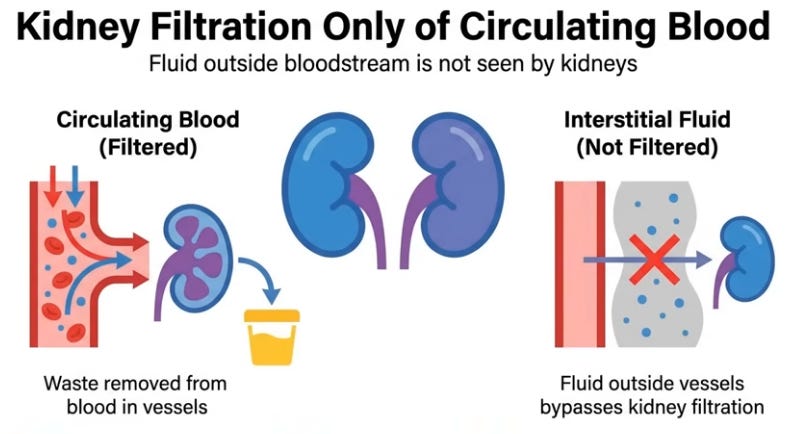
Nocturia, the medical term for repeatedly urinating at night, is not a normal part of aging at 40, 50, or even 70; a healthy body produces antidiuretic hormone (vasopressin) at night, acting like a factory manager instructing the kidneys to concentrate urine, reduce volume, and operate in economy mode, allowing uninterrupted sleep for seven or eight hours. When this mechanism fails, it’s a serious issue: one nighttime trip is a warning, but two or more triggers spikes in pulse and blood pressure, interrupting deep sleep where the brain clears waste, repairs neurons, and the heart rests truly, leading over years to hypertension, depression, accelerated brain aging, and cardiovascular stress worse than smoking, backed by clinical studies. Patients often self-diagnose—men blame their prostate, women menopause or infections—and chase symptoms with teas, antibiotics, supplements, or severe fluid restriction, going to bed parched yet still waking at 3 a.m., because they’re treating the symptom like taping over a fire alarm instead of extinguishing the fire. The bladder is merely the sensor signaling a deeper issue elsewhere; in 80% of cases, it’s healthy, faithfully emptying what’s delivered to it, while the real culprits are the legs and heart filling it overnight.
Rare Red Flags Requiring Immediate Medical Attention
Before exploring mechanisms, recognize urgent symptoms demanding a doctor’s visit over a video: blood in urine without pain {hematuria} signals potential bladder cancer in those over 50, warranting cystoscopy; painful blood in urine suggests kidney stones or infection; bone pain with unexplained 10-20 lb weight loss indicates malignancy; acute retention with straining and abdominal ache is an emergency needing catheterization. If these don’t apply, relief is possible, but protecting sleep quality requires understanding the malfunction type.
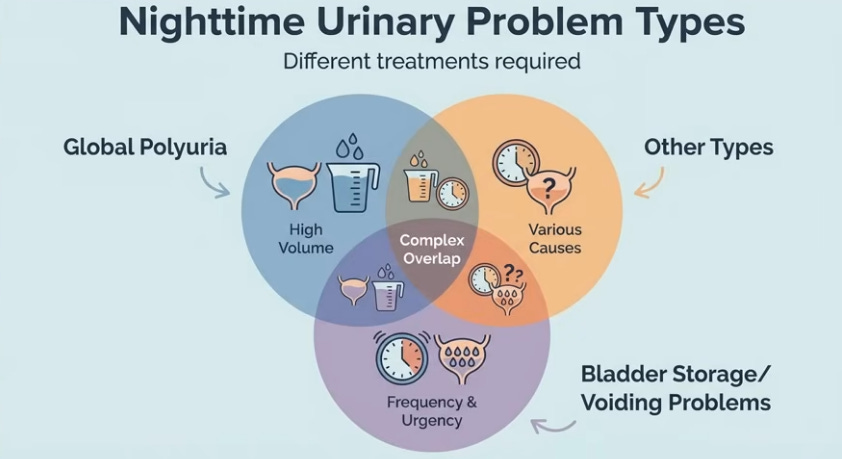
3 Types Nighttime Urinary Problems
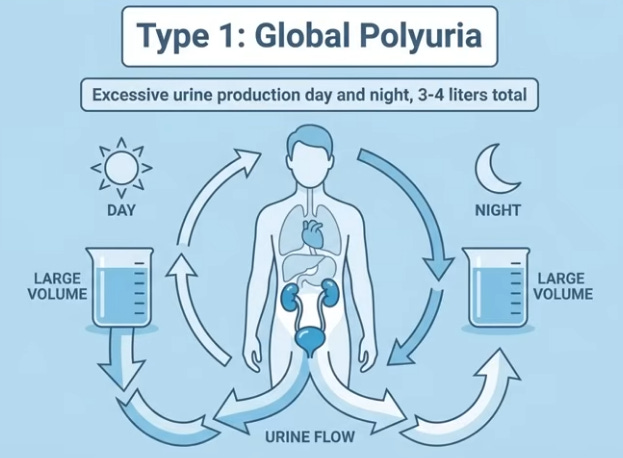
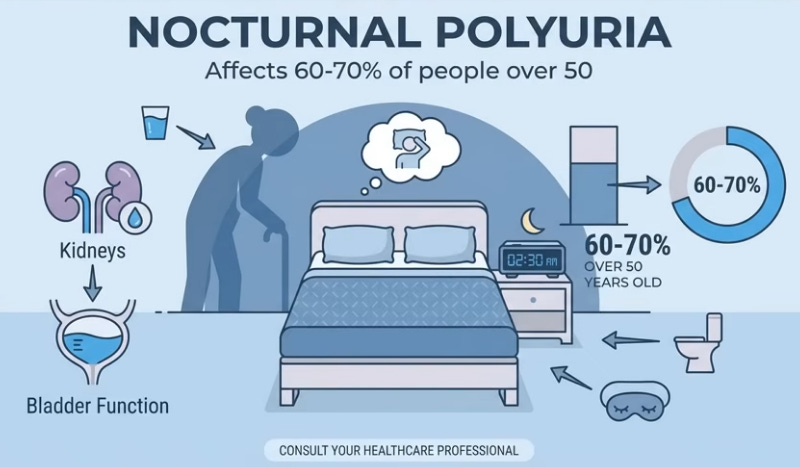
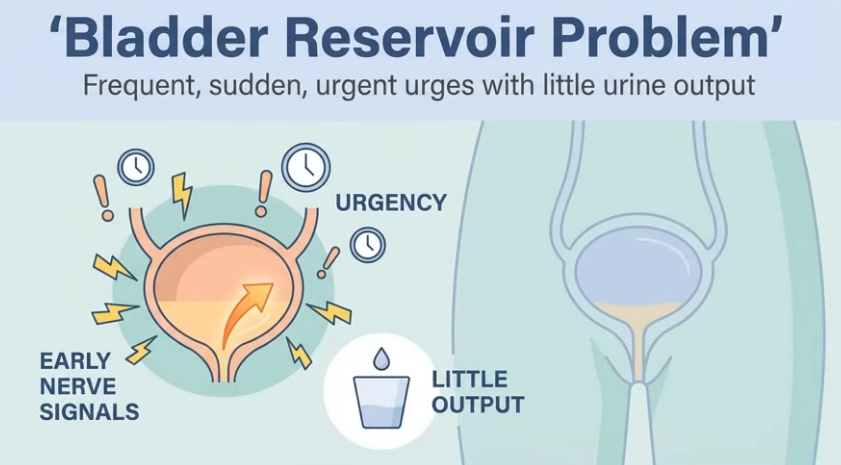
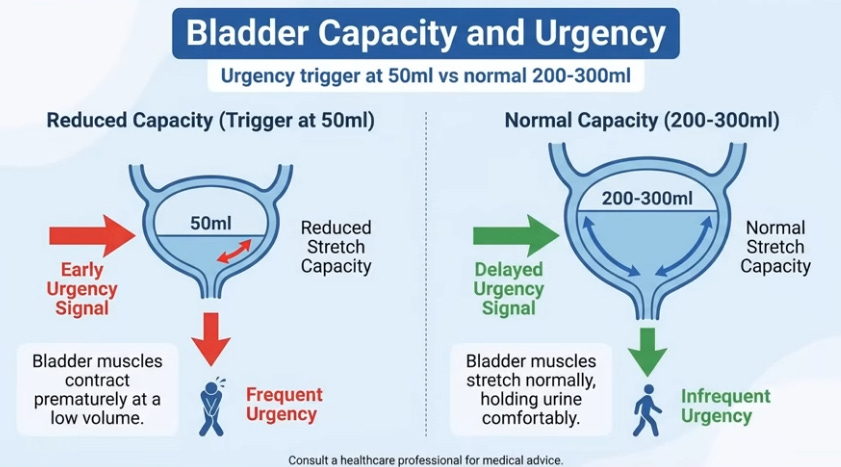
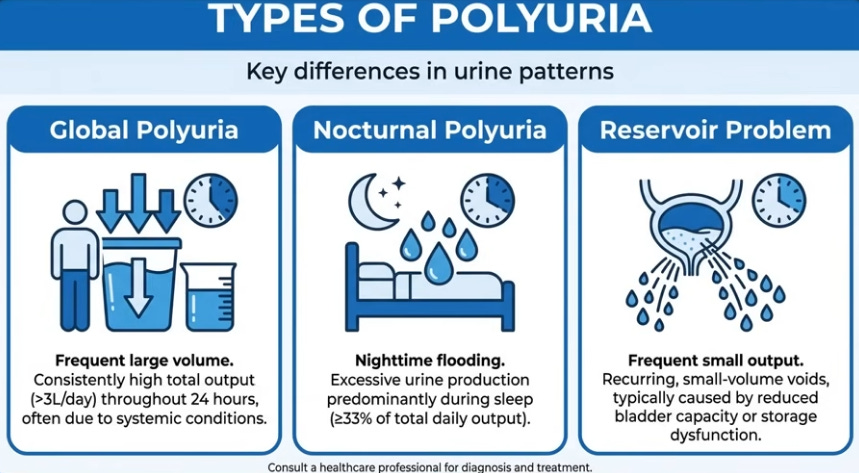
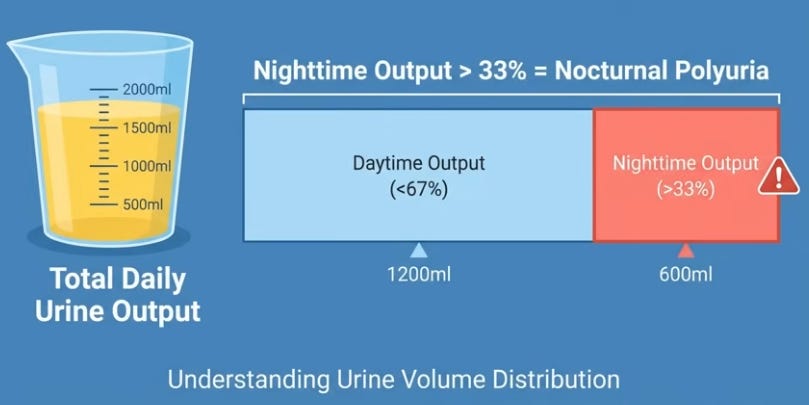
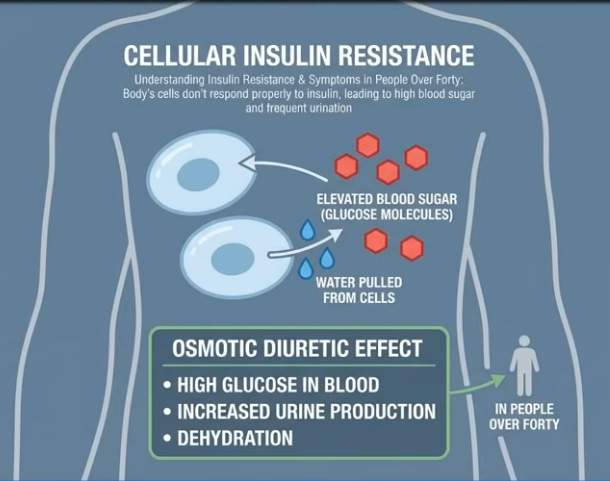
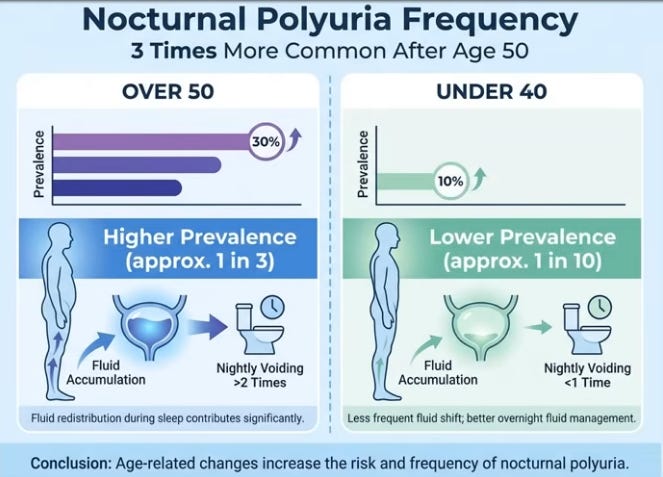
Urology classifies nighttime issues into three types with distinct treatments: Type 1, global polyuria, involves excessive overall urine (3-4 liters/24 hours) from overdrinking or diabetes (type 2 or insipidus), with pale, frequent voids day and night needing endocrine evaluation. Type 2, nocturnal polyuria (60-70% of over-50s), is insidious—normal daytime but nighttime flooding despite low evening intake—as kidneys shift to night mode. Type 3, reservoir dysfunction, features urgent, frequent small-volume voids from overactive bladder, prostate enlargement, infections, or stones; bladder can’t hold 200-300 ml normally. Identify yours: large volumes day/night (global), normal day/flood night (nocturnal), urgent tiny amounts (reservoir).
Anatoli’s Story: A Classic Case of Misdiagnosis
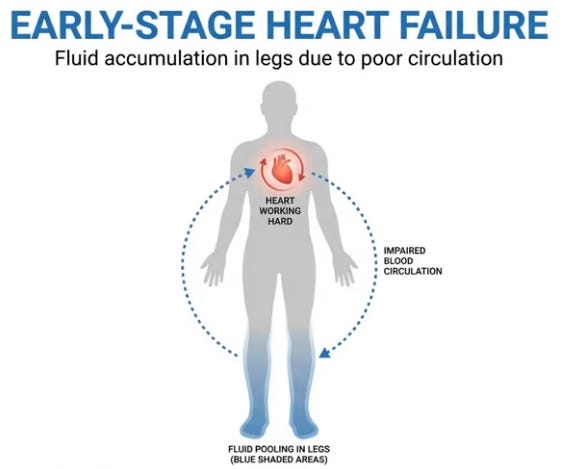
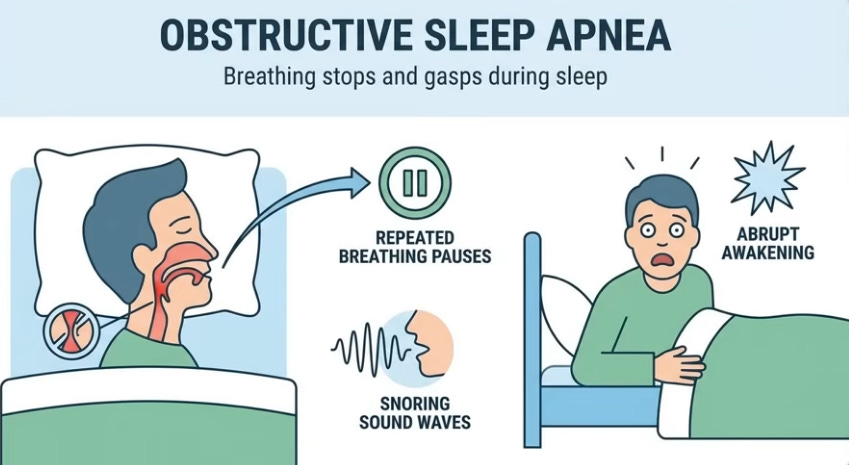
Consider Anatoli, a 54-year-old stoic man desperate after months of 4-5 nightly trips despite prostate supplements, suppositories, and post-6 p.m. fluid ban leaving him thirsty yet releasing half-liters at 2 and 4 a.m.; labs showed normal PSA, mild prostate enlargement insufficient for symptoms, clean bladder. Probing lifestyle revealed leg sock grooves, ring tightness, stair breathlessness from past smoking; diagnosis shifted to early heart failure causing leg pooling and sleep apnea disrupting vasopressin. Supplements targeted the wrong issue—like fixing a faucet amid a basement flood.

The Physics of Leg Edema and Nighttime Flooding
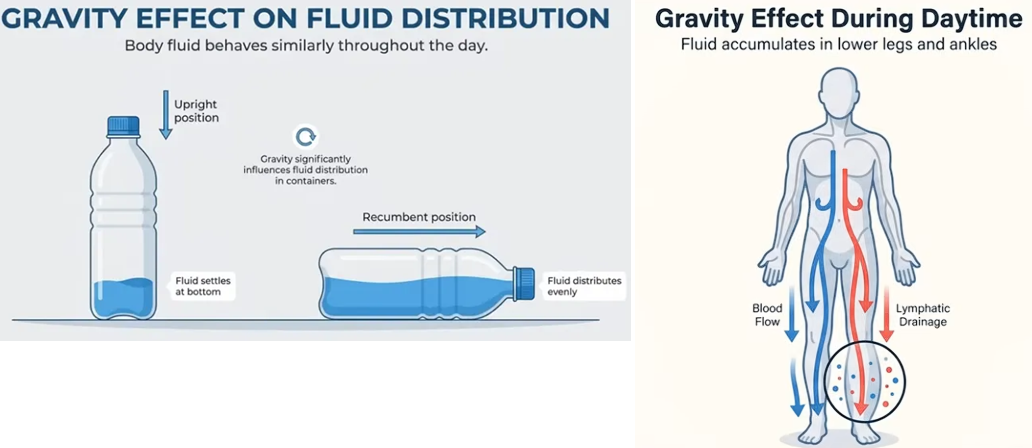
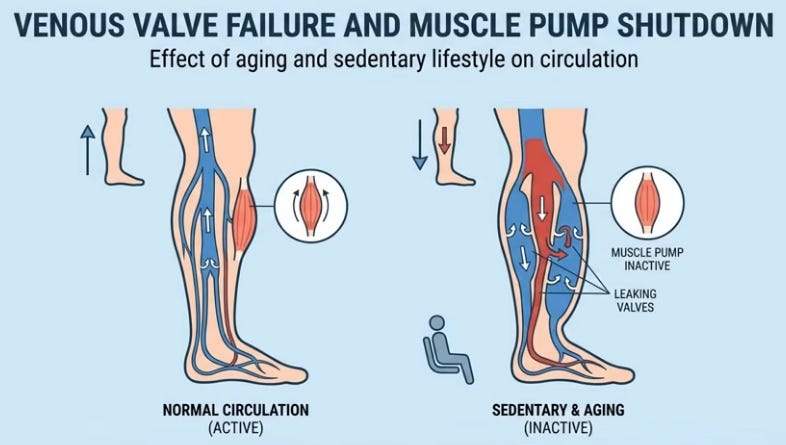
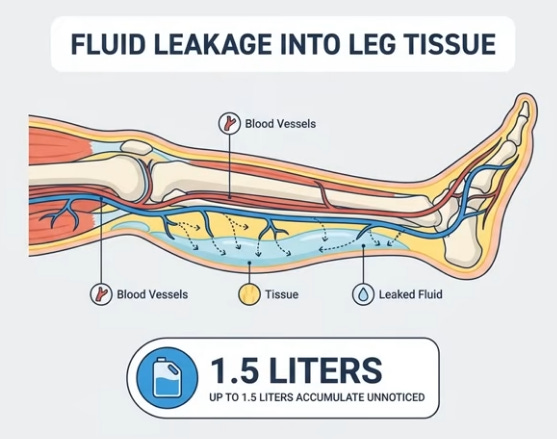
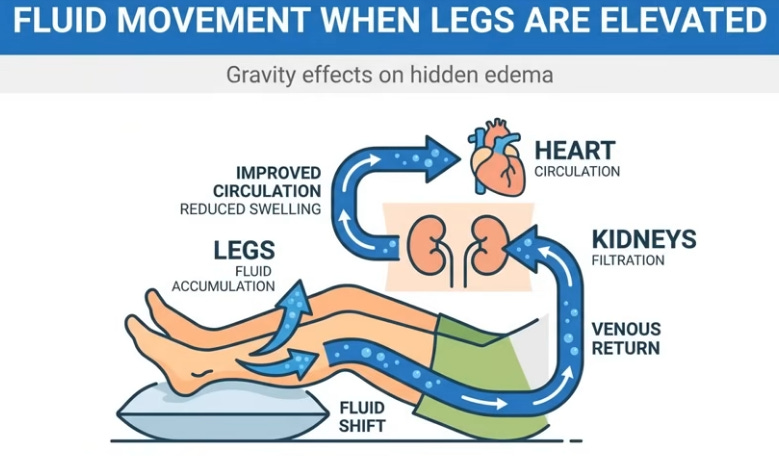
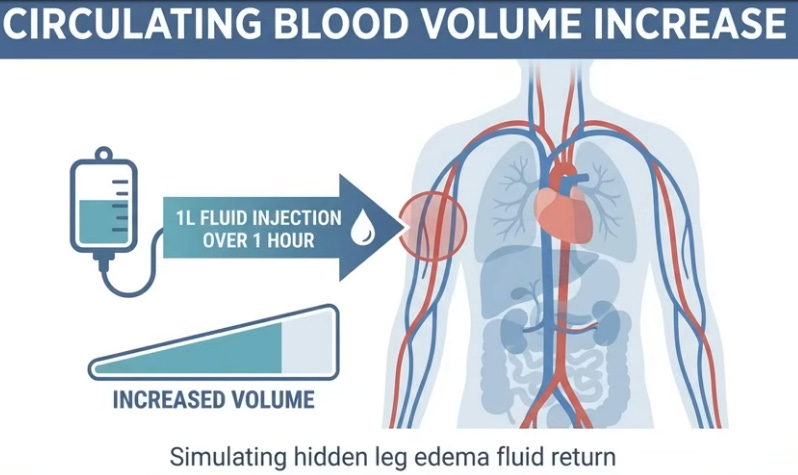
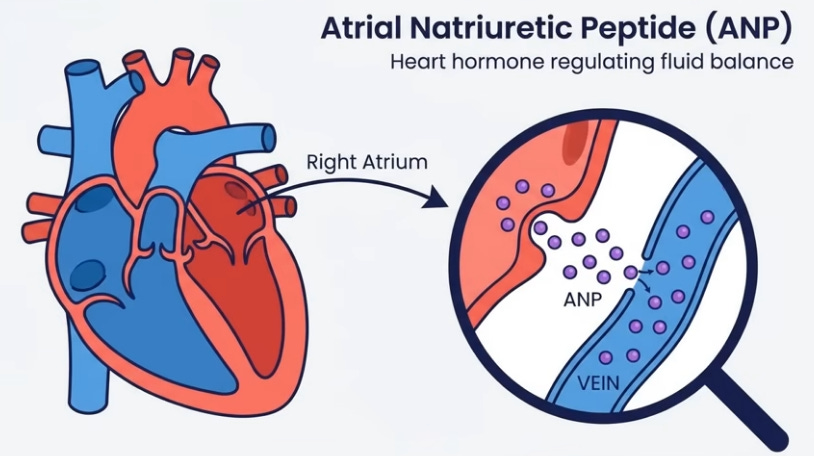
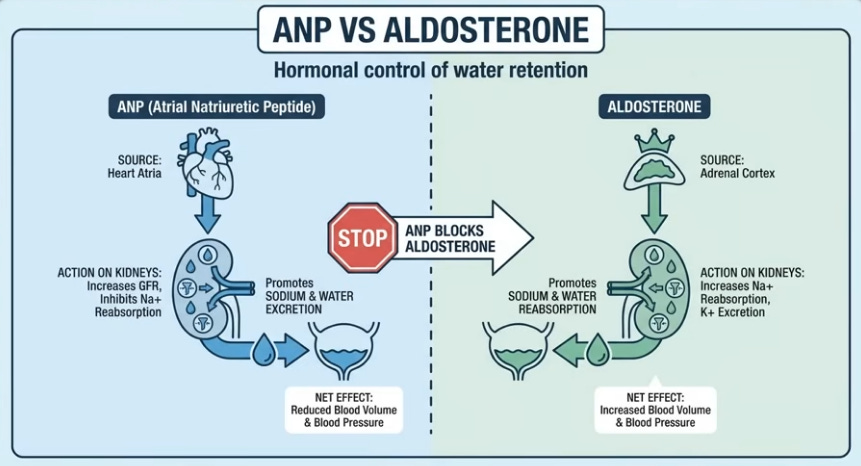
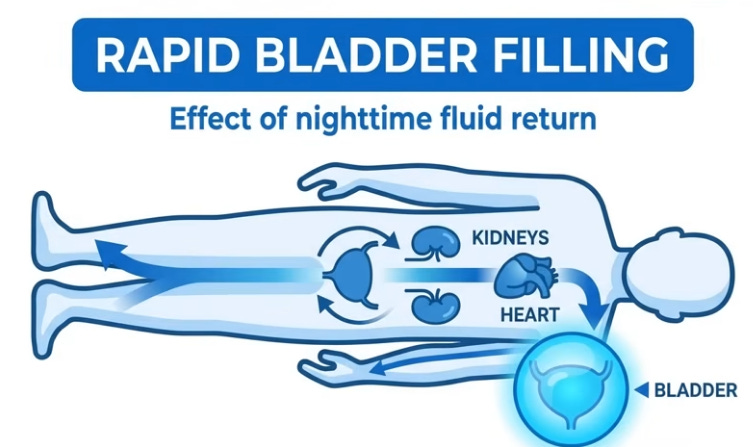
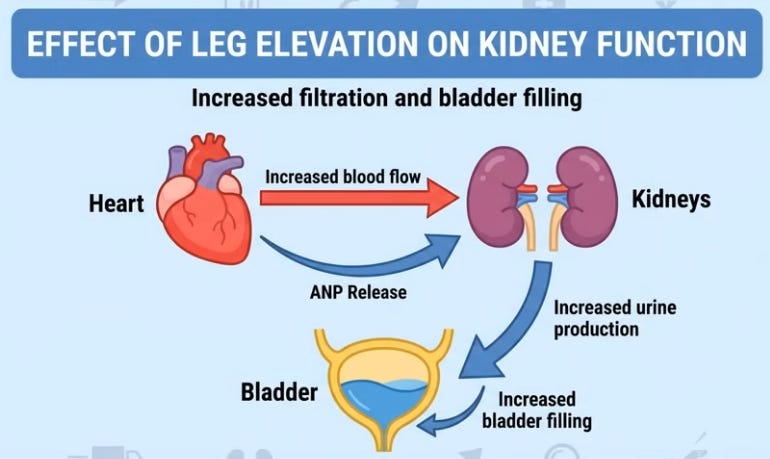
Like water in a bottle shifting when laid flat, 16 vertical hours pool blood, lymph, and interstitial fluid in legs via gravity; youthful elastic veins and muscle pumps resist, but age/sedentary life weakens valves, leaks fluid (up to 1.5L) unnoticed beyond sock marks. Evening salt-heavy dinners exacerbate; lying down levels legs with heart/kidneys, reabsorbing fluid spikes blood volume, stretching the atrium to release atrial natriuretic peptide (ANP), blocking water retention and forcing kidneys to dump fluid/sodium urgently, filling the bladder hourly despite no intake—legs literally “drinking” for you.
Simple Self-Tests for Hidden Edema
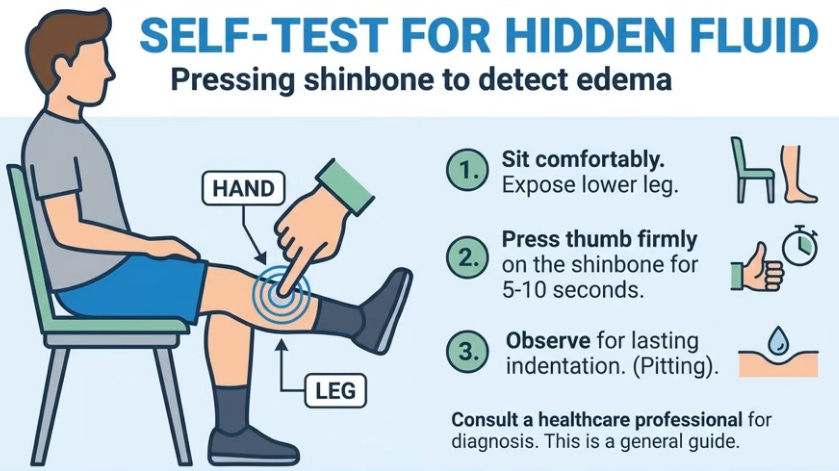
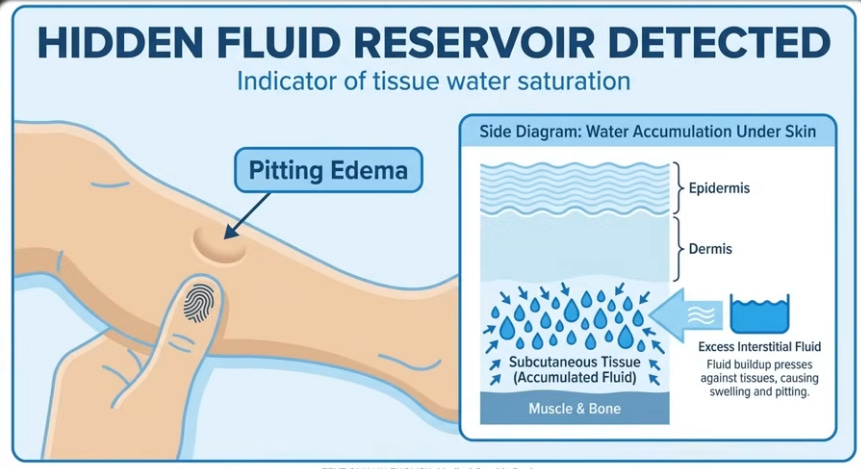
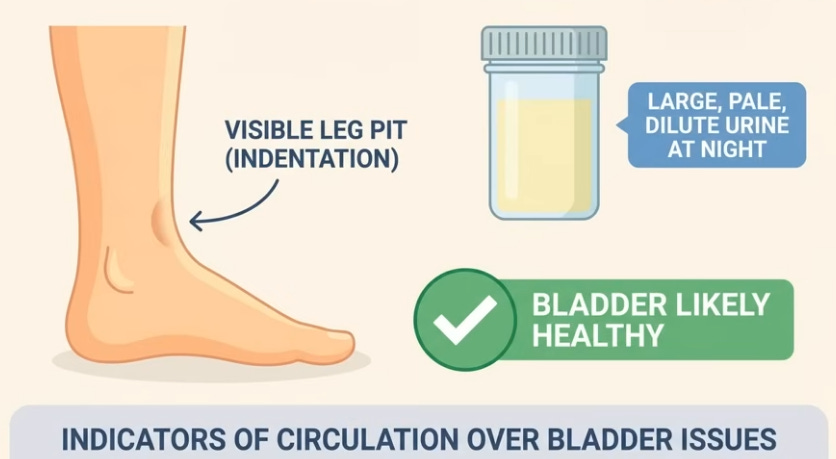
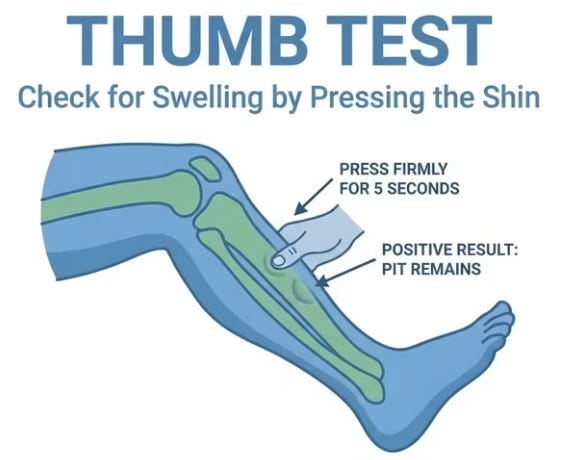
Test 1: Press thumb on shin bone (knee-ankle) 4-6 inches above ankle for 10-15s; lingering pit indicates saturated tissues. Test 2: Track 24h urine; >33% nighttime (e.g., 500ml of 1500ml) confirms nocturnal polyuria from redistribution. Positive tests mean focus on circulation, not bladder.
Dietary Enemies and Allies for Bladder Calm
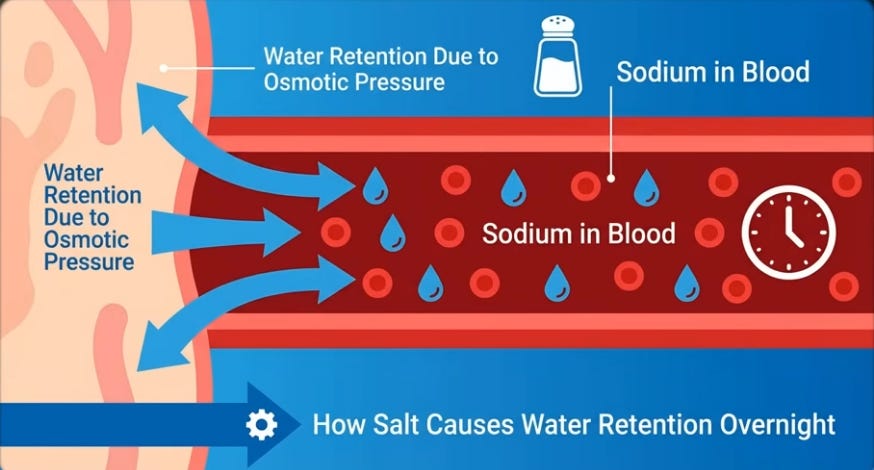
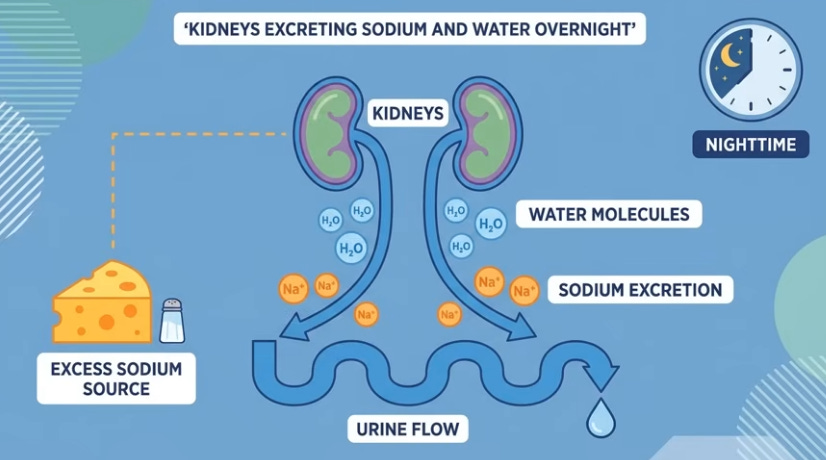
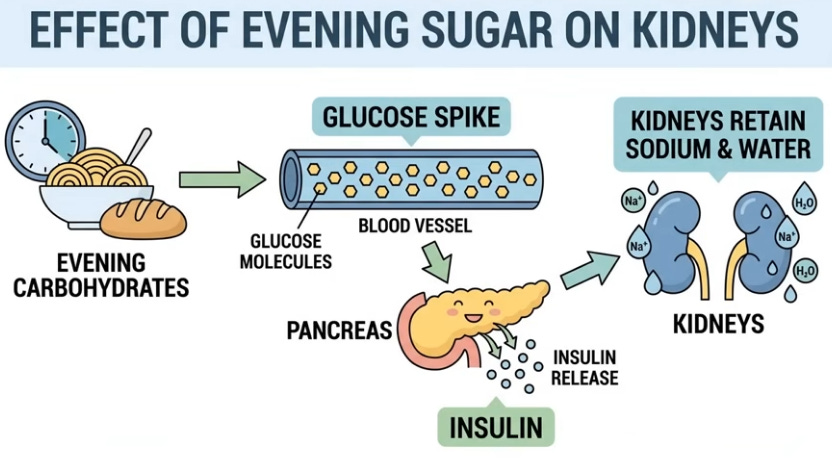
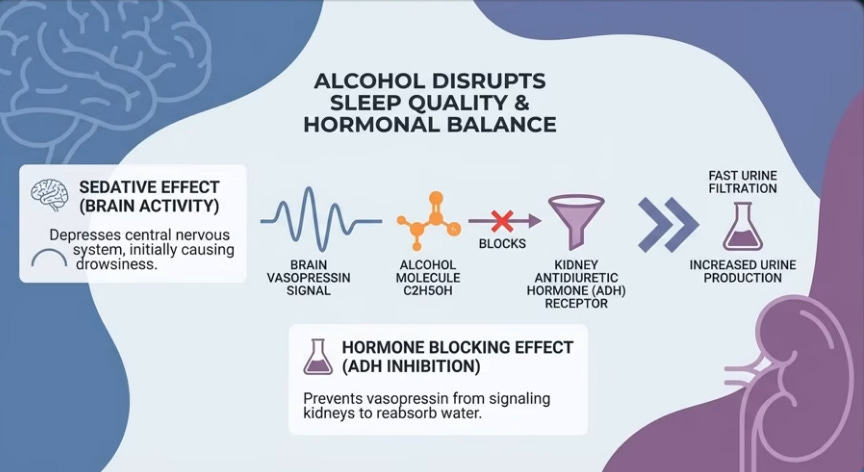
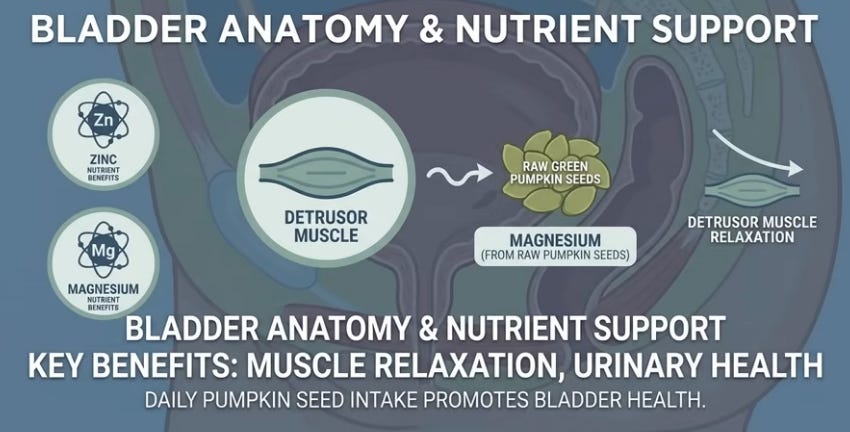
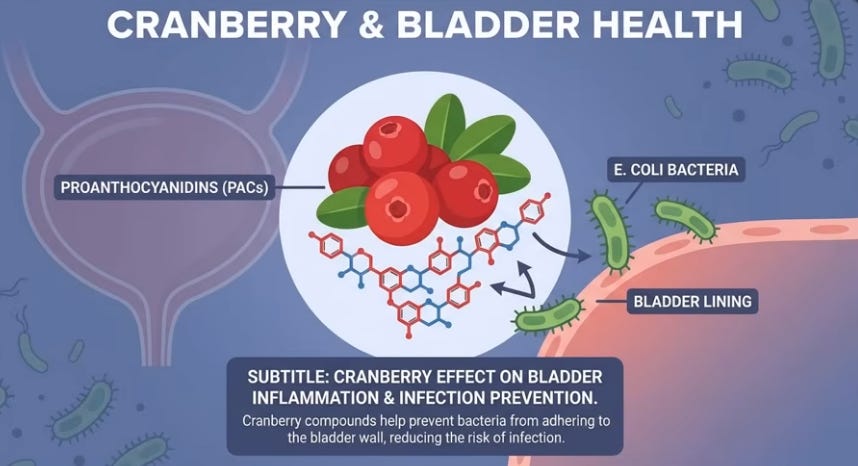
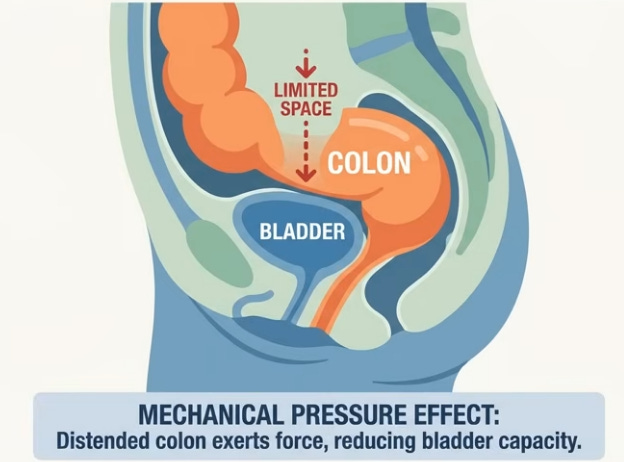
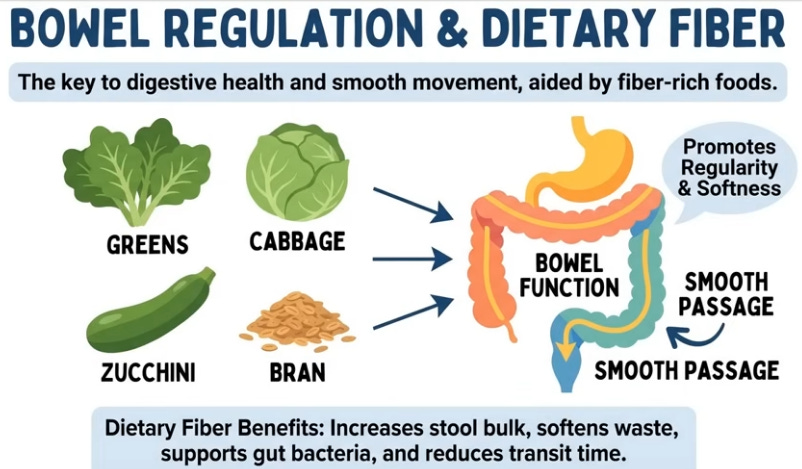
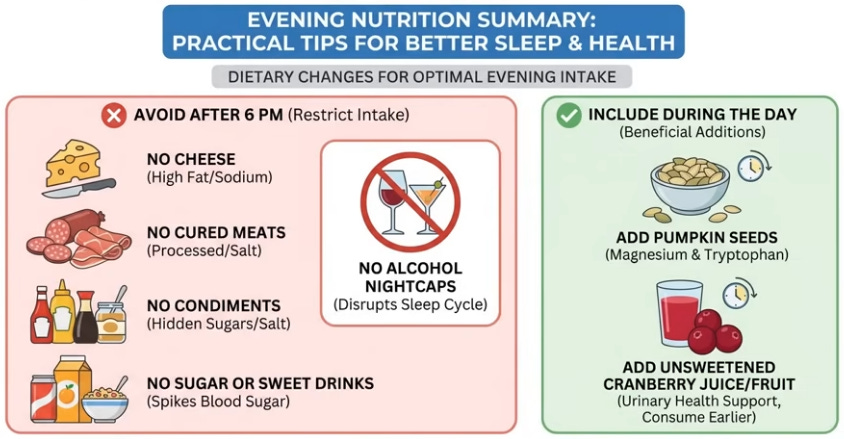
Evening hidden salt (80% from cheese, meats, mayo—100g cheese = chip bag sodium) triggers retention then overnight excretion pulling water; sugar spikes insulin/sodium hold, rebound diuresis, osmotic pull; alcohol sedates but blocks vasopressin for unrestricted filtration, worsening bursts. Allies: 30g raw pumpkin seeds (zinc/magnesium relax detrusor, phytosterols support pelvic floor); unsweetened cranberry (proanthocyanidins block bacteria irritation); fiber (prevents colon pressure on bladder). Anatoli’s switch cut one trip.

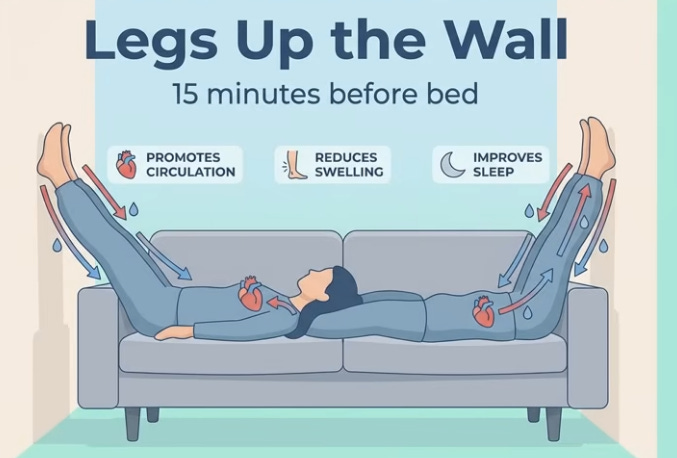
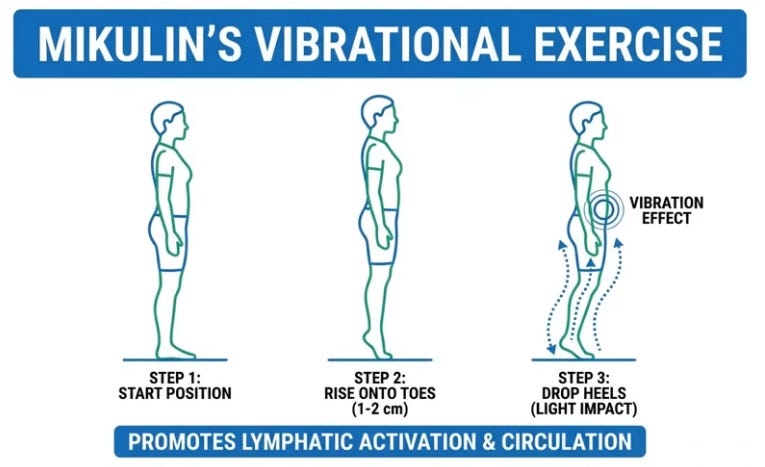
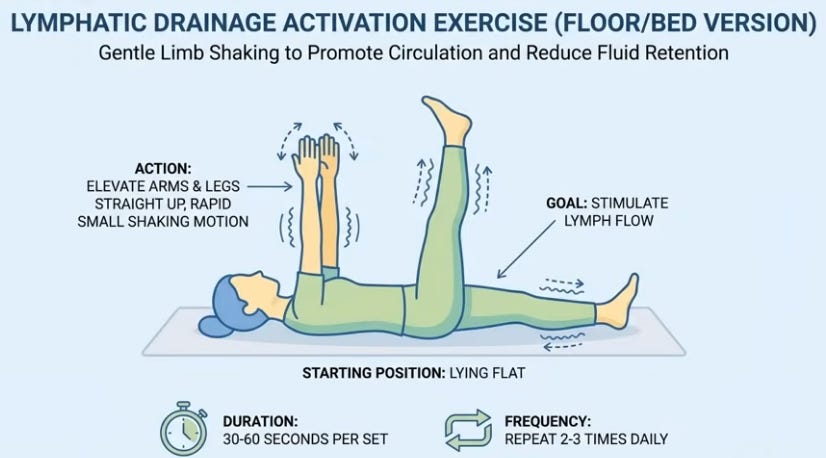
The Golden Protocol: Morning, Day, Evening Routine
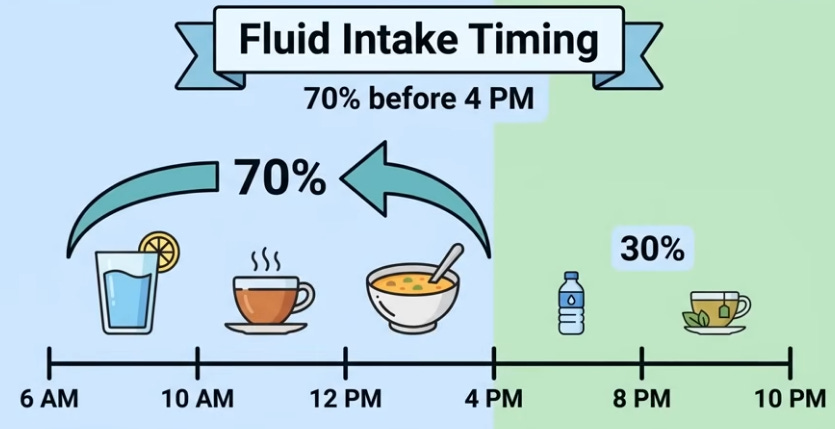
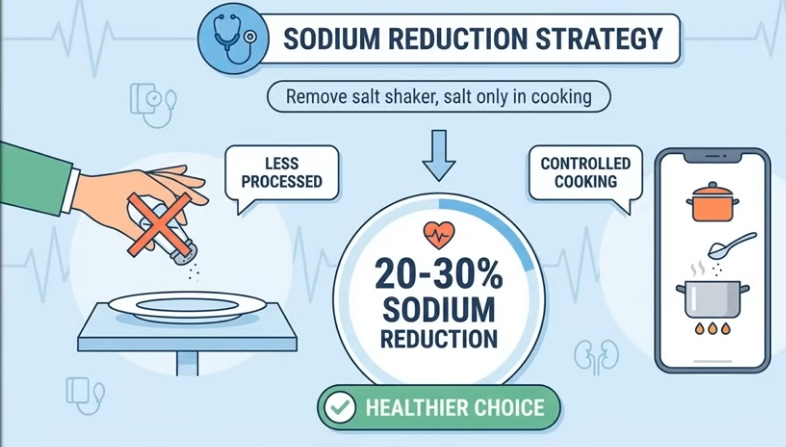
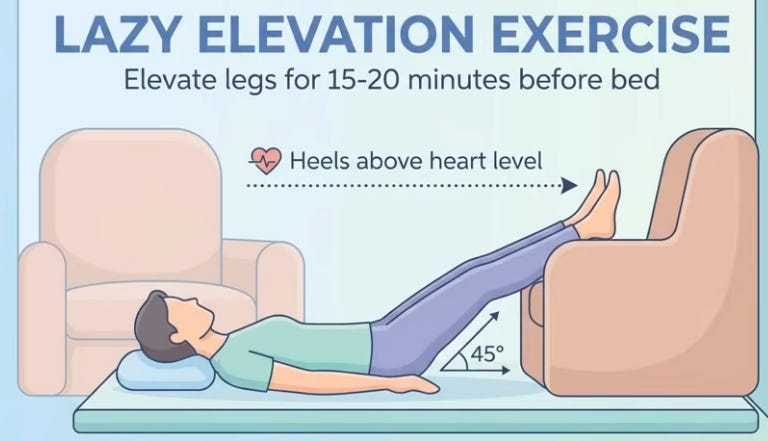
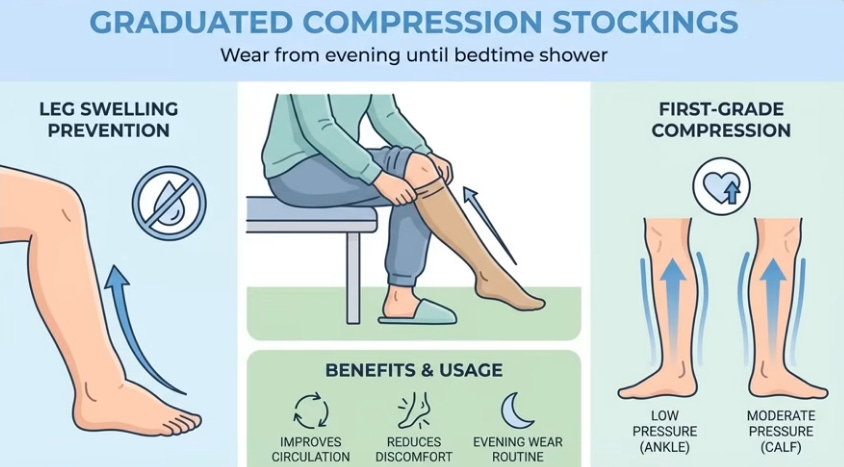
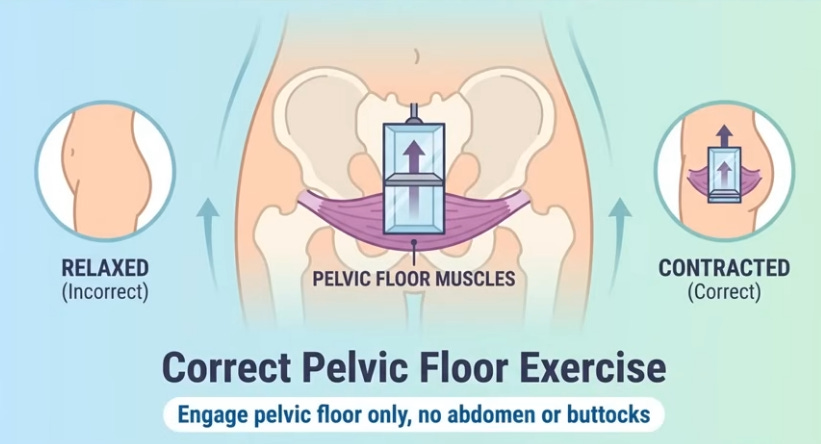
Morning: 30 heel drops (toe rise/drop for calf vibration activating vein valves) or bed leg/arm shakes for lymph. Day: 70% fluids pre-4 p.m., table salt ban (cook only, cuts 20-30% intake). Evening: 1-1.5h pre-bed, 15-20min legs elevated >heart (45° on couch/wall) to preemptively drain 300-400ml while awake; compression stockings if swollen; bed Kegels (20-30x pelvic floor “elevator” holds, abdomen relaxed). Anatoli slept through after consistency; cardiologist noted leg/heart improvement.
Age Factor, Takeaways, and Final Advice
Nocturnal polyuria—excess nighttime urine production affecting 60-70% over 50—triples in prevalence post-50 due to aging vein/valve weakening, causing subtle leg edema (1-1.5L fluid pooling daytime) that floods kidneys upon lying down, triggering wake-ups. Tonight, test via shin pit-press (thumb dent on lower leg), urine diary (>33% night output), salt-free dinner (skip cheese/meats), 15-20 minute leg elevation {Mikulin’s vibrational exercise} before bed (drain while awake), and 20-30 Kegels (perineum squeezes). Leg pit + breathlessness? See cardiologist first for heart or sleep issues; bladder is just signaling—fix root causes physiologically, not symptoms.
{DO THE FOLLOWING TONIGHT}
{MEASURE URINE OUPUT AT NIGHT <1/3 OF DAYTIME OUTPUT}