


HEART DISEASE
Polyunsaturated Fats Are A Major Cause

The following is from a video by Dr. Mason on Atherosclerosis, which is a prominent form of heart disease. It means clogged blood vessels. Sugars, unsaturated fats, and various meds are shown to be the primary causes. I transcribed the talk and divided it into paragraphs and titled each paragraph for convenience.
CONTENTS
CALCIFICATION & PLAQUE RUPTURE.
Dr. Paul Mason - 'The Clotting Theory of Atherosclerosis and Seed Oil Toxicity (updated)'
CLOGGED BLOOD VESSELS.
I'm Doctor Paul Mason. And today I'm going to challenge everything you think you know about this disease, atherosclerosis. You've been told that high LDL levels coat the insides of blood vessels, in much the same way that a drain gets blocked by fat. That's just absurd. Higher LDL cholesterol levels, in fact, are associated with longevity. The overwhelming finding of this systematic review of 19 cohort studies with more than 68,000 participants was that the higher the LDL cholesterol level, the lower the chance of death. The fact is though, LDL particles can be and are found in atherosclerotic plaques, so does that mean it causes atherosclerosis? No. The fact is, as shown by this paper, 75% of patients hospitalized for heart attack do not have higher LDL levels.
BLOOD VESSEL CLOTTING.
Rather, we have compelling evidence that the root cause of heart disease is actually this, a blood clot, or more specifically, thrombosis. Essentially, atherosclerosis is the result of blood clots forming inside blood vessels. To begin with, red blood cells contain a chemical unique to them called glycophorin A. This chemical is not found in any other tissue in the human body. And yet, scientists have been able to prove the presence of glycophorin A, and by extension, red blood cells, deep inside atherosclerotic plaques, by using a special brown stain. Of course, blood clots are not just made of blood cells, they also contain platelets and fibrin, which forms fibrous strands binding the clot together. And both these two have been found buried deep inside atherosclerotic plaques. The lipid hypothesis model of heart disease cannot explain this at all.
CHOLESTEROL V. PHYTOSTEROL.
What about the cholesterol light crystals that we see in plaques? Where do they come from? Well, it doesn't come from LDL. The cholesterol found in atherosclerosis comes from red blood cells. You see, their outer membrane contains more cholesterol than any other cell in the body. And this paper not only describes the central accumulation of red blood cell membranes within atherosclerotic plaques. It also tells how, by injecting red blood cells into animals, investigators were able to produce atherosclerotic plaques that contain both cholesterol crystals and LDL-laden foam cells. So blood clots can elegantly explain the constituents of atherosclerotic plaques, all of them. So I'd like to now take a closer look at the so-called cholesterol crystals themselves. Phytosterols are plant molecules almost identical to cholesterol. And they do form crystals, which are difficult to differentiate from cholesterol crystals. And phytosterols can be easily delivered by red blood cells, given that they can actually be incorporated into the membrane of red blood cells, and cells, in the same way that cholesterol is carried in the red blood cell membrane. Phytosterols are readily detected in atherosclerotic plaques.

PHYTOSTEROLS & OILS.
Fortunately for most of us, our bodies reject most of the phytosterols that we consume with only about 1% being absorbed and assimilated into our tissues. Some people, however, are unlucky enough to absorb much larger amounts of these plant sterols, between 15 and 60%, and this condition is called phytosterolemia and the consequences can be dire, there being one case of a 5 year old dying from sudden cardiac death. Despite this, these phytosterols are often lauded for their ability to reduce cholesterol levels, which is why products such as this containing plant sterols are actually perversely promoted for cardiovascular health, despite there being approximately zero evidence of cardiovascular benefit, and significant evidence of harm. And this is where seed and vegetable oils need to come into the conversation, both of which contain significant amounts of plant sterols, even olive oil. This shows the plant sterol content of oils. While olive oil and coconut oil are not generally considered seed oils, because they're made from flesh, they still contain phytosterols. So this study looked at the impact of three fats and found that both coconut and olive oil resulted in a drop in LDL levels. In my opinion, this was due to their phytosterol content, as the coconut oil was 94% saturated fat, a clear repudiation of the claim that saturated fat increases LDL.

{Carbon=carbon double bonds are prone to oxidation. In saturated fats above there are no carbon=carbon double bonds, but unsaturated fats have one, two, or 3 each. So unsaturated fats are less stable and oxidize quickly.}
OXIDIZED OILS.
Now, one of the major reasons seed oils contribute to atherosclerosis is that their polyunsaturated chemical structure contains unstable bonds which are prone to oxidation. Basically, all the seed and vegetable oils you see in stores are oxidized, and fish oil is too {because it is nearly 80% unsaturated fat}. This study found that oxidation of all walnut oil occurs within days of it being produced. And when oxidized oil is consumed, oxidation products are absorbed and enter the body. The more oxidized the oil, the higher the level of blood oxidation products. The story for blood oxidation products becomes even more interesting in subjects with poor blood sugar. The two left columns here represent subjects with normal blood glucose levels and the right column those with poorly controlled diabetes. You can see that the blood oxidation product level is much higher after consuming oxidized oil in the poorly controlled diabetics. Furthermore, the oxidation products persisted for three days in the diabetic subjects, while being cleared in eight hours in the non-diabetic subjects. So what, you might ask, is a problem with oxidation products in the blood? The answer is atherosclerosis. Oxidative stress in the blood causes clotting, or thrombosis, which is the source of atherosclerotic plaques. In the words of this paper, oxidative stress is involved in all of the major processes leading to thrombosis. So we're now starting to understand why atherosclerosis happens.
OXIDATION & CLOTTING.

So what is oxidation? It's basically an umbrella term that refers to a chemical reaction where an electron is ripped away from a molecule. And this is basically what rusting is. And because of this reactive tendency, oxidation products in the blood can activate clotting factors. Of course, seed oils are not the only source of blood oxidation products. Pollution is a major one. When we inhale pollutants, if they're small enough, they can pass through the blood vessels in our lungs, and enter our circulation. And this has been proven by research, detecting pollutant particles within just one minute of inhalation. This is why smoking causes heart disease, as in the case of President Eisenhower, who was smoking two or three or more packs a day. Of course, some pollutants are worse than others. Remember when petrol used to fill the air with lead for us to inhale? Well lead is a particularly potent contributor to oxidative stress. Lead atoms are just the right size to be inhaled and enter our circulation. And this study from 2018 concluded that one in six deaths, or 18% of the 2.3 million deaths occurring in the United States every year, was attributable to lead. A huge number. And remember that all comes back to oxidation products in the blood.
NORMAL V. OXIDIZED LDL.
But just how exactly is oxidation carried around in the blood? What does it look like? How about an LDL particle? Yeah, I did say people with higher LDL levels on average do live longer. But LDL particles can become oxidized when they react with other oxidized substances. You see, normally in the blood there's a single healthy population of LDL in a normal distribution, as shown by a single peak here in yellow in the LDL section. The size and density though of LDL changes when it becomes damaged, of which oxidation is a major cause. In this sample you can see 4 distinct populations of LDL, three more than normal, representing the presence of oxidized and damaged LDL, and this LDL is often referred to as small dense, given that, as they oxidize, the LDL particles become microscopically smaller. And while most people who have heart attacks have normal total levels of LDL (there being no difference in the total LDL levels in those with and without heart attacks), when we look at oxidized LDL, it's a different story. Look at the level of damaged LDL in the age group on the left without heart disease, compared with the two groups on the right with heart disease. Night and day.
GLYCOCALIX DAMAGE & CLOTTING.

Oxidized LDL, of course, or any other blood oxidation product, is able to damage this furry layer which lines our blood vessels, called the glycocalyx. And the glycocalyx is perhaps the most important level of protection against atherosclerosis that most people, doctors included, have never heard of. It creates antithrombin-3 that inhibits clots from forming and stimulates the production of nitric oxide, itself another potent inhibitor of coagulation. The fact that oxidized LDL damages our glycocalyx significantly increases the risk of atherosclerosis.
CALCIFICATION & PLAQUE RUPTURE.
And oxidation stress, too, appears to be the cause of calcification within arteries. That coronary artery calcification is associated with heart attack is therefore probably not a coincidence. Interestingly, statins are also known to damage DNA, an effect apparent to the Japanese scientists who stopped researching the mycotoxin, which eventually became the first statin, because of the increased rate of cancer in dogs, which makes it unsurprising that statins also significantly increased coronary artery calcification. This ties in with the most common cause of sudden heart attacks. Which is not the presence of atherosclerotic plaques themselves, but rather with the plaques rupturing. High calcium scores indicate an increased tendency for atherosclerotic plaques to rupture. In the case of the rupture of an existing atherosclerotic plaque, the resulting thrombus that forms can be so large that it completely occludes the vessel, resulting in a heart attack.
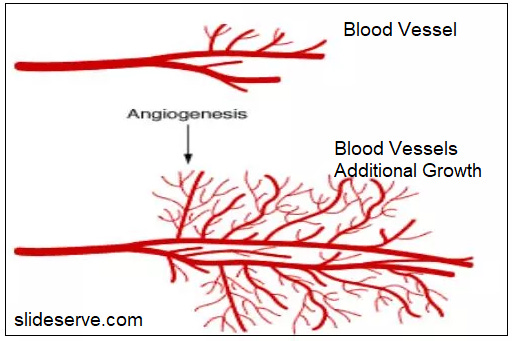
Atherosclerotic plaques themselves, though, while narrowing arteries, do not usually lead to complete occlusion. They restrict flow, but they don't completely obliterate it. This then affords the opportunity for something called angiogenesis, or the creation of new blood vessels. Essentially, when a blood vessel becomes too narrow to carry the desired volume of blood, new blood vessels can be created, as a detour around the restriction. This is why a coronary artery calcium scores are a much better predictor of cardiac death than vessel narrowing itself, because they reflect the stability of the plaque or its tendency to rupture and form an occlusive thrombus. This study, for example, found that once calcium scores exceed 100, representing the presence of unstable plaques, it doesn't matter whether or not blood vessels are narrowed. The risk of cardiac events or death remains the same. Essentially, if your calcium score is over 100, the data suggests that invasive angiograms where dye is injected so the outline of blood vessels can be seen is largely pointless. So what's going on inside a plaque to make it susceptible to rupture in the first place? Well, it depends mainly on the integrity of the fibrous cap. The question is what causes the fibrous cap to thin out? Foam cells secrete enzymes that break down connective tissue, like the protective cap over the atherosclerotic plaques. These are called matrix metalloproteinases, and these enzymes have been independently associated with both the tendency of plaques to rupture and cardiac mortality.
USELESS STENTS.
This is why stenting the blood vessels to open them up also doesn't improve survival in heart disease symptoms such as angina. Stenting doesn't eliminate the risk of sudden blockage, which in fact is actually what kills people. This study, published in 2007, randomized 2287 patients with heart disease, and stenting was shown to be of no benefit. More recently, this 2020 study randomized 5179 patients with heart disease, and again, it found absolutely no mortality benefit to stenting.
DIABETES & ANTIOXIDANTS.

There's another elephant in the room, of course, when it comes to heart disease, and that's diabetes, which is associated with the tripling of the risk of death from heart disease and stroke. That high levels of sugar in the blood are so problematic has been known for a long time. This research from 1962 demonstrated glucose abnormalities in 73% of heart attack patients. And again, the mechanism is oxidative stress. Both high and especially fluctuating blood glucose levels generate oxidative stress at the level of the mitochondria, the consequences of which you saw earlier when combined with seed oil consumption, with oxidation products detectable in the blood for three days in diabetics. That's a very good reason to keep your blood glucose level in check. The corollary of all of this is that oxidation is a major cause of heart disease and that antioxidant supplements may be beneficial. For example, the antioxidant acetylcysteine has been found to be protective against heart disease, as has the antioxidant coenzyme Q10.
UNSATURATED FAT STUDIES.
I'd like to now finish off the discussion about seed oils. I believe the evidence of harm from seed oils is convincing enough to discourage their consumption. The consumption of seed oils began to rise in the early 1900s, well-timed to have a causal role in the heart disease epidemic. And it's not just this association that suggests their consumption is problematic. Four randomized controlled trials have demonstrated harms from consuming seed oils. In this study from 1965 patients post heart attack were randomly allocated to one of three groups. There were two intervention groups consuming a daily supplement of either olive or corn oil and a control group on a regular diet, and after two years, 75% of the subjects in the control group remained free of repeat heart attack, compared to 57% and 52% of those in the olive and corn oil groups, respectively. Hardly a ringing endorsement for olive or corn oil. The conclusion of the investigators was quite blunt, being that corn oil cannot be recommended for the treatment of ischemic heart disease. And in my opinion, this study also raises questions about olive oil.
FAT STUDIES ON MEN.
Now the City Diet Heart Study was a randomized controlled trial examining the effect of replacing saturated fat with polyunsaturated fat in men that had heart attack. But despite being finished in 1973, the results regarding whether the intervention reduced cardiac mortality were destined to never actually be published. And it was only after doctor Chris Ramsden uncovered the raw study data on punch cards and magnetic tapes in a basement, that the full results were finally published some 40 years later. The key finding being that the increased intake of polyunsaturated fats as found in seed oils increased the risk of death in these men by 62%. A similar story exists for the Minnesota Coronary Experiment, which also finished in 1973. Now this was a double blinded randomized controlled trial on more than 9000 men and women, again evaluating the effect of increasing polyunsaturated fats. And again, there was an inexplicable delay in publishing the full findings. It took 16 years to publish a somewhat redacted version of the study findings. And again, a very similar story. The mortality data from the Minnesota Coronary Experiment, which was completed in 1973, was not published until 2016. And when the results were finally published 43 years later after the raw data was located by Doctor Chris Ramsden, that same chap again, it was revealed that increased seed oil intake increased the chance of death, a result that was knowingly hidden for decades. And when the now-deceased late author was asked about this delay, he explained it was because they found the results disappointing.
FAT STUDIES ON WOMEN.
Now more recently, we have the Woman's Health Initiative study, published first in 2006. It was a massive study of over 48,000 females designed to definitively assess the benefits of lowering saturated fat and increasing polyunsaturated fat intake. And the most important outcome clearly was that of survival. And while the results were technically published, they were done so in a very obscure, some would say suspicious, manner, almost like the authors didn't want anyone to actually see them. This vague sentence on page 661 of the publication was the single reference to the only statistically significant finding of the whole paper, the finding being that females with a history of heart disease faced a 26% increased chance of complications like heart attack, if they followed a low saturated fat diet. Furthermore, the most recent published data on the Woman's Health Initiative demonstrates that this risk to the low fat intervention group has only increased over time to between 47 and 61% increase risk. The last few years have seen various people debate as to whether seed oils, or carbohydrates, are worse for health. And I think the answer is both. Although it does depend on the dose. Take for example this British Medical Journal paper, which found that, in terms of percent energy intake, diets exceeding 6% seed oils were more harmful than diets containing 50% or more carbohydrates. Based on the fact that the average Australian derives 13% of their energy from seed oils, it would seem that seed oils are indeed more problematic on a population basis.
CLOTTING THEORY ORIGIN.

Now I'll acknowledge the work of Scottish GP doctor Malcolm Kendrick on exposing the role of blood clots in atherosclerosis. Here's the author of this book, which provides an excellent summary of the clotting theory. And it's also the subject of cancellation by Wikipedia, accused and convicted by online editors of being a fringe figure with the audacity to argue against the lipid hypothesis. Outrageous.
INSLUIN RESISTANCE.

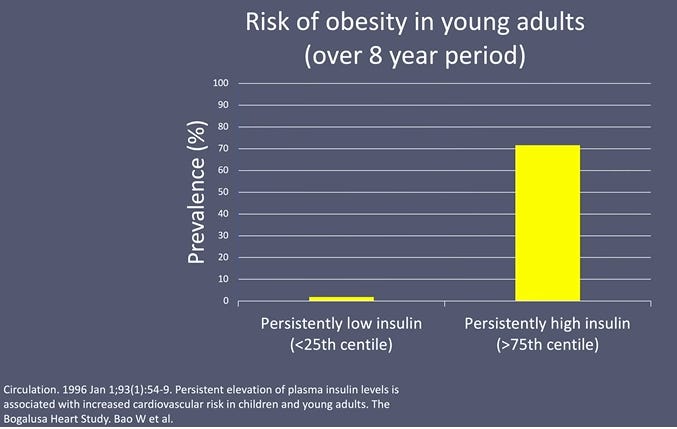
I'd like to briefly present something for the first time publicly, my theory on the mechanisms of insulin resistance. How can it be caused both by sugar and seed oils? In actual fact, I believe the mechanism by which seed oils and sugar causes insulin resistance is near identical. And this also explains why statins make it worse. In this six year study, insulin resistant subjects developed cerebrovascular disease, type 2 diabetes, coronary heart disease, cancer and hypertension. Equally striking is his research on insulin resistance and obesity. Only 2% of the subjects with the least insulin resistance became obese over eight years. Compare this with the 72% of the most insulin resistant subjects: 36 times greater.

So what exactly is insulin resistance? One function of insulin is to remove glucose from the circulation and place it into muscle, liver and fat. Insulin resistance, however, means that the insulin is less effective and notably, the liver is most affected. This results in the liver not receiving glucose as it normally would. Because muscle has a finite capacity for how much glucose it can store under the influence of increased insulin levels, fat tissue now receives more glucose. Now, the key to understanding the cause of insulin resistance is to realize that it's not caused by a problem with insulin itself, but rather by the receptors upon which insulin acts. Which makes sense because the state of insulin resistance is usually associated with higher levels of insulin.

So I wondered whether I could find any evidence of any mechanisms by which both excess sugar intake and seed oils could impair the functioning of the insulin receptor.
FRUCTOSE & SUGAR.
Now we've got an abundance of evidence linking fructose sugar with insulin resistance. Several experimental studies found that simply by reducing fructose intake, insulin resistance was rapidly reversed. 41 children had their fructose intakes reduced from an average energy proportion of 12% to 4% while maintaining their total level of energy consumption and, after just nine days, there were large improvements in insulin resistance, not to mention a 47% reduction in liver fat after just nine days. The reverse is also true. Increasing sugar consumption induces insulin resistance. In this study, 80 subjects were randomized to either more than two or more than four servings of fruit a day, and after six months, the group consuming the most fruit along with all of that extra fructose were significantly more insulin resistant. Now, to understand how sugar causes insulin resistance, we need to come back to the structure of a cell, which is surrounded by a membrane, known as the phospholipid bilayer, and embedded within the bilayer are insulin receptors, which span the thickness of the cell membrane. When insulin binds to the receptor, the receptor is activated and passes its message into the cell, upon which the downstream actions of insulin take place. If this receptor doesn't work, you'll have a state of insulin resistance, where insulin seems to not work properly.

The missing link in understanding insulin resistance comes down to the fact that the phospholipid bilayer is in fact not a homogeneous ocean of phospholipids. Rather, it is punctuated by little islands recently discovered, known as lipid rafts, which float within {or on} the cell membrane. These lipids are actually below the resolution of light microscopy and contain large amounts of cholesterol, three to five times that of the surrounding membrane, and insulin receptors are embedded within these lipid rafts. Anything that disrupts the lipid raft can disrupt the function of the insulin receptor. It's well-established that excess dietary fructose results in the overproduction of a waxy lipid molecule called ceramide. And ceramides not only disturb lipid raft function, but they've also been proven to lead to insulin resistance.
OILS & CELL LIPID RAFTS.
What about seed oils though? This 1965 paper provides the earliest account I've found of seed oils causing insulin resistance. It describes the experience of two subjects, who were ultimately removed from the study, assessing corn oil supplementation. One subject developed glucose in the urine, a classic symptom of diabetes. The corn oil was then stopped and the glucose disappeared from the urine. The corn oil was then resumed, at which point the glucose returned. Eventually, the investigators finally stopped the corn oil supplement for good. The other subject was also noted to have developed diabetes, based on the glucose tolerance test, only a few weeks after commencing the oil supplement. Now recall that seed oils contain large amounts of these sterols, the fake plant cholesterol, and sterols have not only been proven to be effectively incorporated into cell membranes, but they've also been shown in some studies to disrupt lipid rafts. Remember too, the high cholesterol content of the lipid raft. Well, depletion of lipid raft cholesterol has been proven to be detrimental to both lipid raft function as well as impairing insulin receptor activation.
STATINS & ANTIPSYCHOTICS.
This is no doubt the reason why the rate of diabetes is significantly increased in people who take statins. And what about the differential impact of insulin resistance on different tissues? Well, as it turns out, there are differences in the lipid raft structure between liver cells and fat cells and this, I believe, explains a differential sensitivity to cholesterol depletion, ceramides and sterols. And all of the literature which I've looked at so far seems to support this notion. It's like I was sitting in this same theatre yesterday listening to Doctor Zoltan talk about how antipsychotic medication causes insulin resistance and diabetes. I thought, well, that was interesting. Let's have a look and see if there's any literature on the topic of lipid rafts and antipsychotic medication. And lo and behold, a quick search later on Google Scholar and there are papers describing how antipsychotic medication disrupts lipid rafts. So basically everywhere I've looked at, the lipid raft seems to be central to the development of insulin resistance. And there is a biologically plausible mechanism supported by literature, describing how both excess sugar intake and seed oil intake can contribute to lipid raft disruption.
AUTOIMMUNITY
{This is from an older video by the same author.}
I mentioned before very early on in our chat about lectins and gluten, some of these proteins which are found in plant based foods can actually cause intestinal inflammation. So if I see somebody with a high homocysteine level, I'll then often do some testing for antibodies that can cause autoimmune disease. An autoimmune disease is when your body starts attacking itself. Normally, if you get an infection, your body will see a virus as foreign and it will mount an immune response against it with antibodies. They're like little guided missiles that will attack that virus. Normally antibodies will target parasites, bacteria, viruses. But if this immune response goes rogue, they might actually target your own healthy cells. And there's very good evidence that these proteins that are predominantly found in plant foods called lectins can trigger autoimmune responses through something called molecular mimicry. And then, once you have this autoimmune response going on, it might attack your thyroid. So I can actually do a blood test and look for antibodies against your thyroid, which might lead to celiac disease. So there's some antibodies we look at, that provide evidence of celiac disease, that might be affecting your pancreas and autoimmune diabetes, which is type one diabetes. It could be affecting your joints as rheumatoid arthritis. So there's a myriad of different antibodies that we can test for. And I'll usually base my selection of those antibodies on symptoms. Do they have joint pain? Do they have abdominal symptoms? Do they have troubles with insulin resistance? Etcetera. When the immune system targets a bacteria, it doesn't actually look at the whole bacteria, it just looks at a molecular signature such as a short sequence of amino acids or proteins or carbohydrates or a short sequence of molecules on the surface. Let's label a sequence as A-C-E and that's able to trigger an immune response because your body says A-C-E is foreign. Then these antibodies are developed to target this A-C-E sequence. The immune system can recognize the same molecular sequence on your cells. That's called molecular mimicry. Your immune system is just confused. I've had a lot of success in clinic with people with low grade nutrient malabsorption. They've got circulating antibodies against the thyroid. Hashimoto's thyroiditis is very common, and probably if we test people in their 60s and 70s, more than 50% of people at that age would have evidence of some antibodies being developed against their thyroid. And that leads to lethargy, fatigue, malabsorption of nutrients. It's also associated with gut inflammation. And when we eliminate some of these foods that have the highest concentration of these problematic lectins, their symptoms usually improve dramatically.
Excellent article, thanks for posting. Ann